Mobitz I occurs when conduction is progressively delayed through the AV node and eventually fails. It is represented by progressively prolonging PR intervals followed by a “dropped” P wave. It does not always represent pathology, particularly when seen in younger or physically fit individuals with high vagal tone.
Second Degree Atrioventricular Block – Mobitz I

Examples
Second Degree Atrioventricular Block – Mobitz I
There is variable decremental conduction through the atrioventricular node (i.e., progressively prolonging PR interval) that ultimately results in a dropped P wave.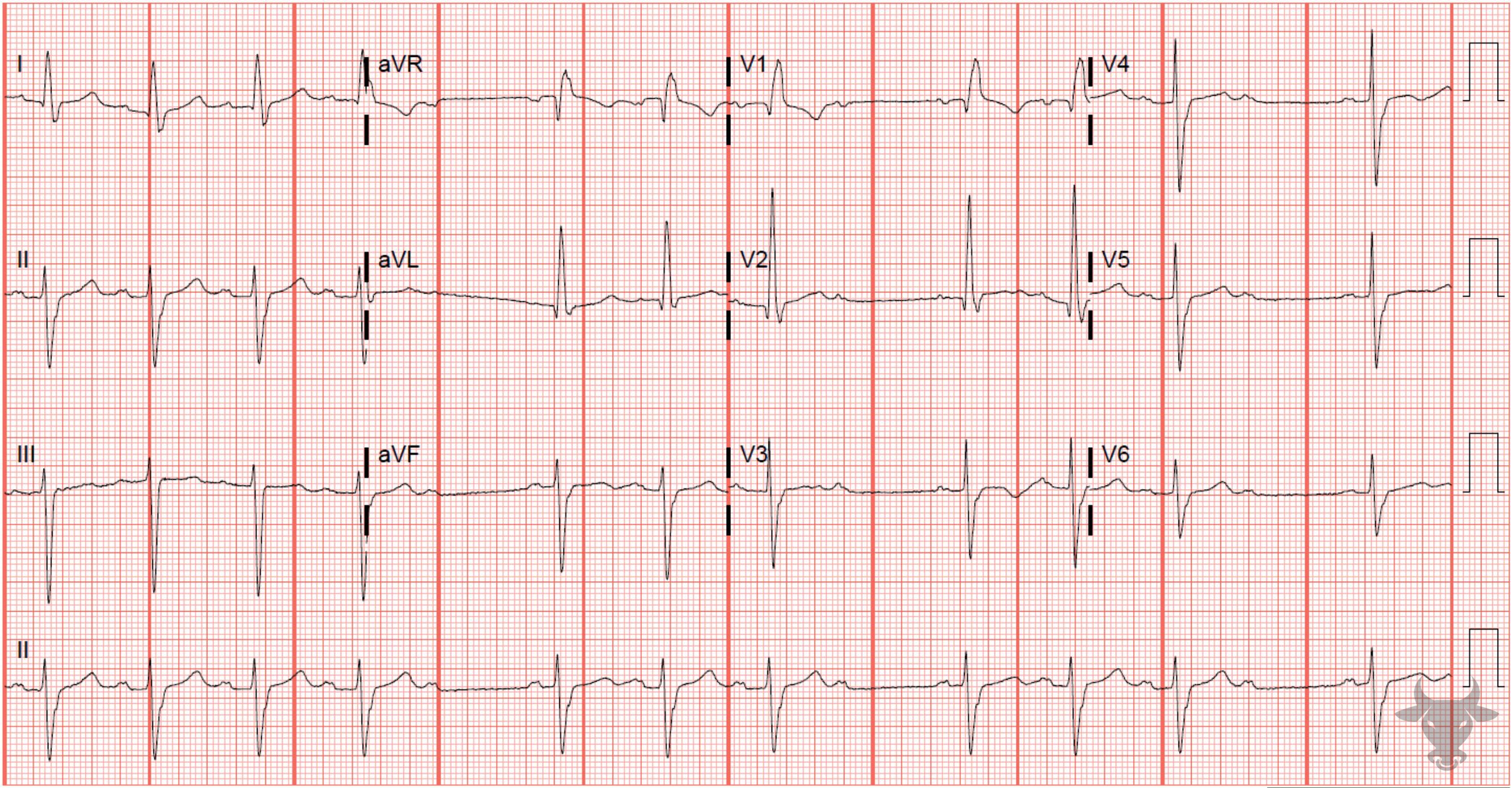
Second Degree Atrioventricular Block – Mobitz I
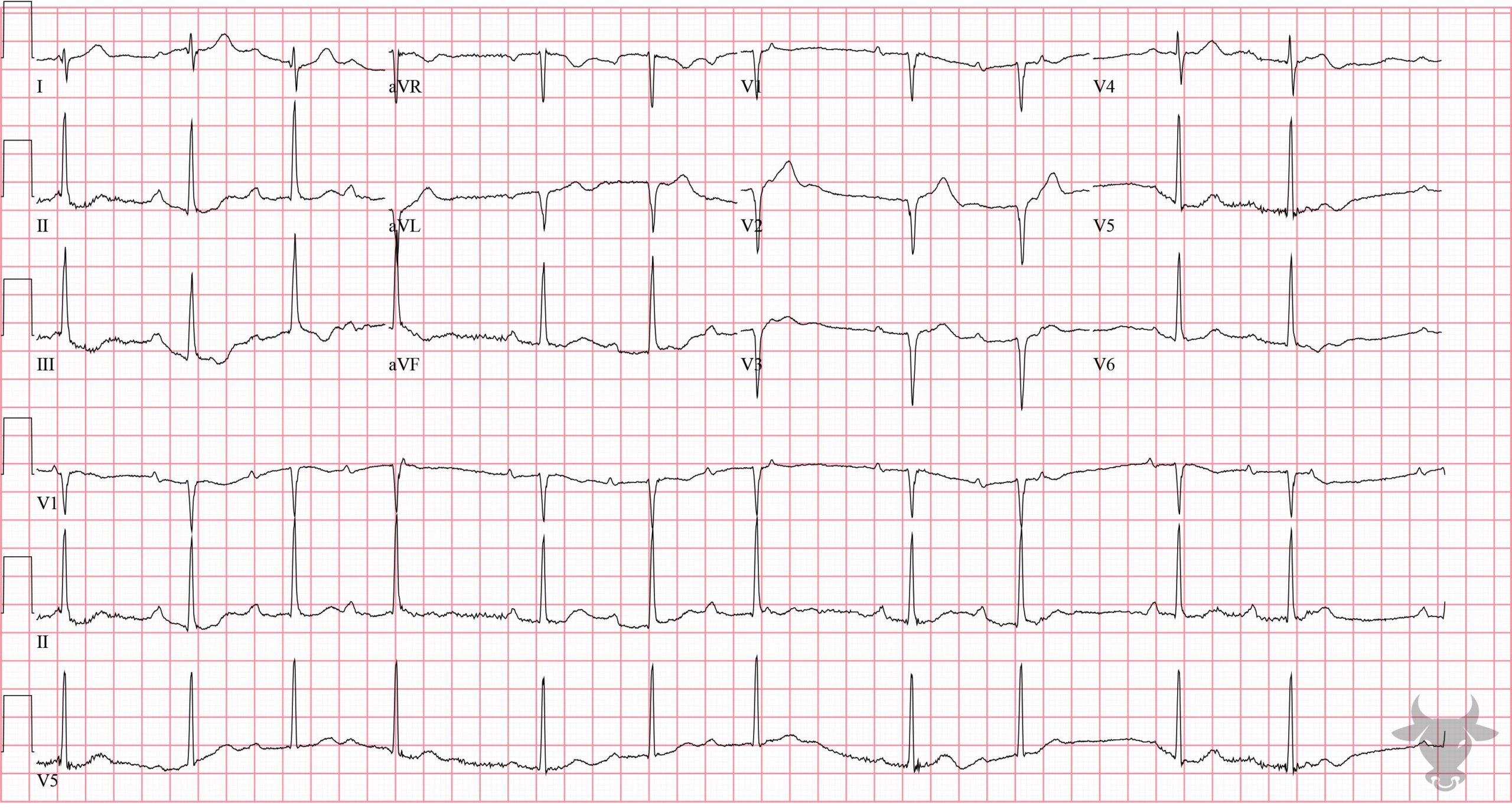
Second degree atrioventricular block, Mobitz I associated with right bundle branch block and left anterior fascicular block. This represents trifascicular disease and the patient is at risk for progression to complete heart block.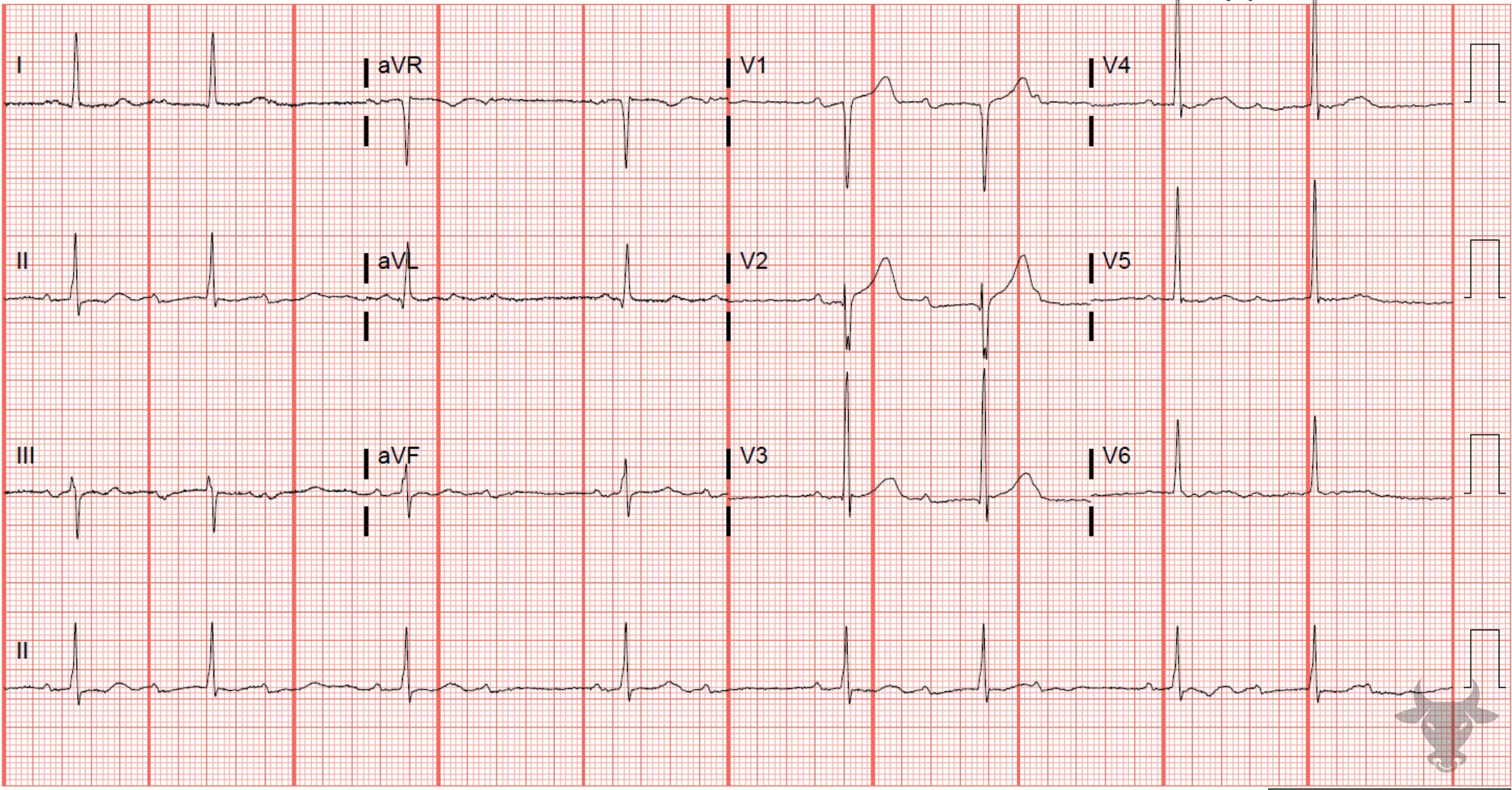
Second Degree Atrioventricular Block – Mobitz I
Conduction is 2:1 at times, but there are two series (one near the beginning and the other near the end) of 3:2 conduction, confirming Mobitz I atrioventricular block.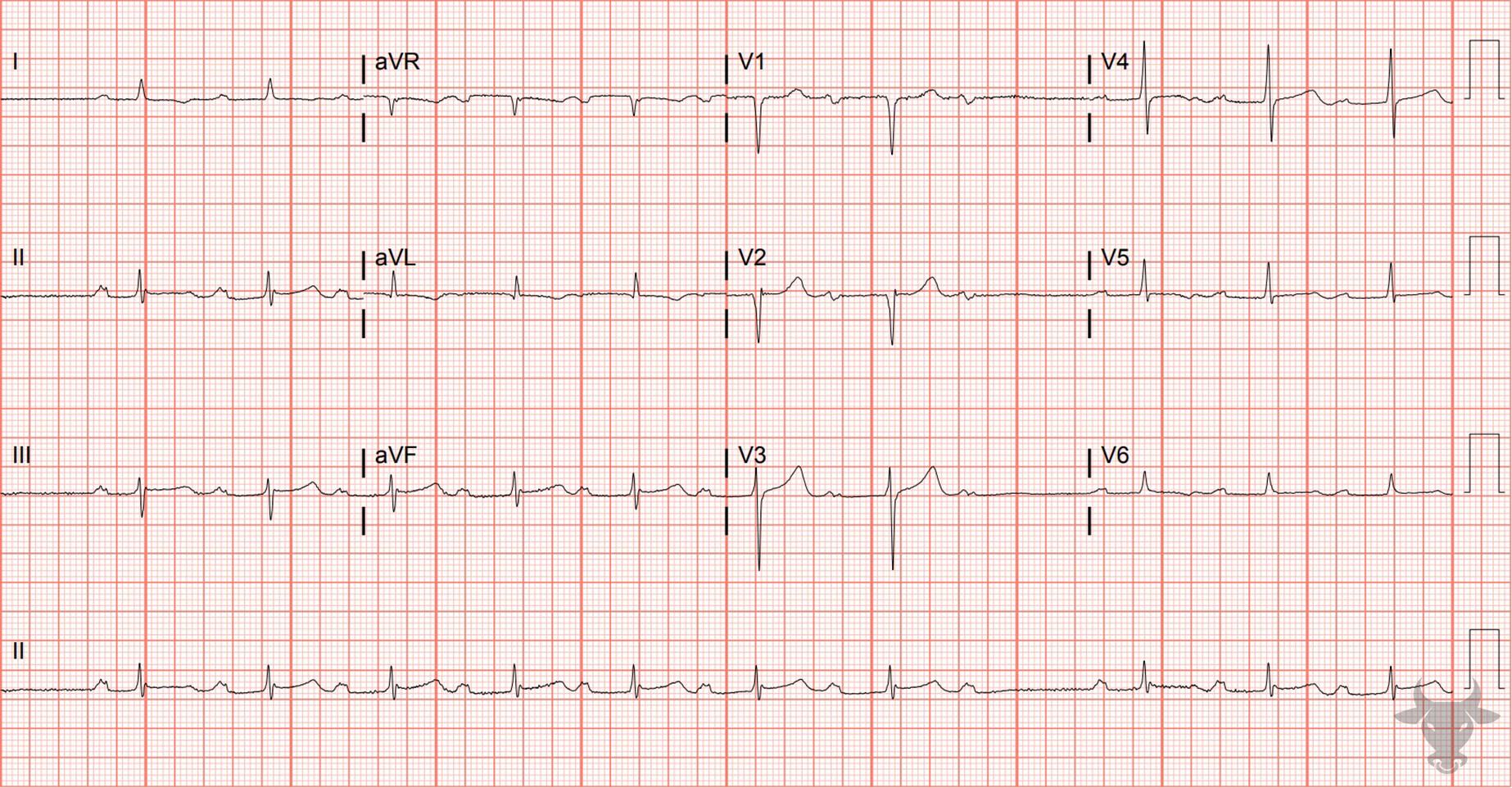
Second Degree Atrioventricular Block – Mobitz I
There is a prolonged PR interval that progressively lengthens until a P wave is “dropped,” or fails to conduct through to the infranodal conduction system, resulting in the absence of an associated QRS complex. This represents 8:7 conduction (i.e., there are 8 P waves for every 7 QRS complexes).References
- Costa D Da, Brady WJ, Edhouse J. Bradycardias and Atrioventricular conduction block. Br Med J. 2002;324(March):535-538.
- de Pádua F, Pereirinha A, Marques N, Lopes MG, Macfarlane PW. Conduction Defects. In: Macfarlane PW, van Oosterom A, Pahlm O, Kligfield P, Janse M, Camm J, eds. Comprehensive Electrocardiology. London: Springer London; 2010:547-604.
- Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhyth. Circulation. 2019;140(8):e382-e482.